By Dr. Julie Gilmour
Prior to Exam
- Hand hygiene, introduce self, informed consent, exposure & draping.
General Inspection
- Ascertain height, weight & BMI
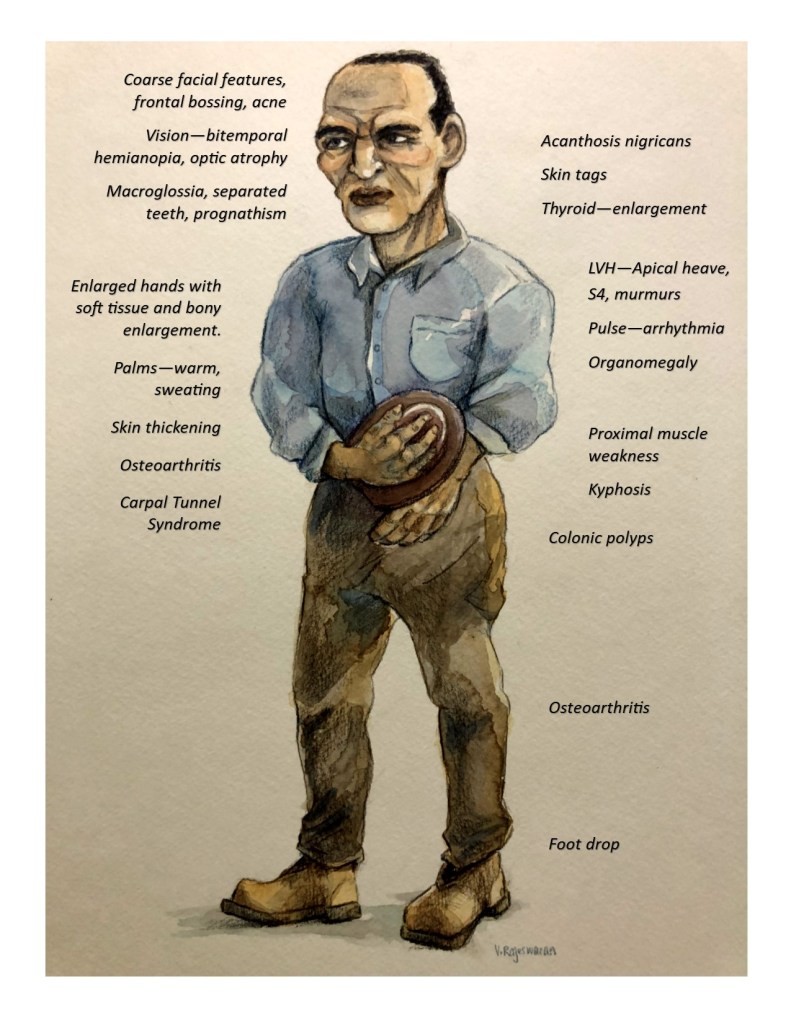
- If GH excess prior to epiphyseal fusion = gigantism
Hands
- Inspection of hands:
- Wide spade-like hand shape (due to soft tissue and bone swelling)
- Enlarged thenar and hypothenar eminences
- Palms – increased sweating and warmth
- Skin thickening
- Measures diameter of middle phalanx of middle finger on both hands
- Done for serial monitoring (middle phalanx less likely to be affected by physical activity)
- Hand volume (immerse to wrist crease in a graduated flask with water)
- Examine for changes of OA (premature)
- Heberden’s nodes (marginal osteophyte at the distal interphalangeal joint)
- Squared thumb
- Examine for carpel tunnel syndrome
- Highest specificity
- Hypoalgesia (decreased sensitivity to pain) in median nerve territory
- Classic or probable Katz hand diagram result
- Weak thumb abduction strength – tests abductor pollicis brevis
- Other tests – Phalen’s test (hold for 60 sec in prayer sign), Tinel’s test & inspect for thenar atrophy
- Highest specificity
Arm
- Measures BP – HTN
- Examines upper arm strength (ie. deltoid) for evidence of proximal myopathy
- Palpate behind medial epicondyle for ulnar nerve thickening
Head
- General facial inspection
- Coarse facial features
- Acne
- Frontal bossing (due to expansion of frontal sinus)
- Eyes
- Assesses visual fields – bitemporal hemianopia if pituitary tumor
- Assesses EOM & visual acuity (see pituitary cranial n examination for details)
- Fundoscopy examination
- optic atrophy – due to CN 2 compression
- papilloedema – due to increased ICP
- angioid streaks – due to degeneration & fibrosis of Bruch’s membrane. Red/brown/grey streaks that are 3-5x the diameter of the retinal vein and emanate from the optic disc (Extra)
- Examine for HTN & DM retinopathy changes
- Mouth
- Macroglossia
- Separated teeth
- Jaw – square and protrudes (prognathism) – secondary to lengthening of mandibular arm
- Hoarse voice (sonorous low pitched, not really hoarse )- due to soft tissue enlargement of the larynx and pharynx ; hoarse if vocal cord polyps develop
- Hirsutism in women
Neck
- Thyroid – examine for diffuse enlargement or multinodular goiter
- Enlarged neck circumference seen with OSA (collar size > 17 inches in men & 16 inches in women) – due to enlargement of larynx
- Kyphosis of thoracic spine
- Skin tags
- Acathosis Nigricans
Chest
- Cardiac Exam
- Palpate carotid pulse – irregular pulse due to arrhythmia (ie. AF)
- Palpation – apex heaving/sustained due to LVH
- Auscultation – increased incidence of valvular heart disease (AR, MR), S4
- Examine for evidence of heart failure – due to diastolic dysfunction and LVH
- JVP (elevated), auscultate lung bases (crackles), pedal edema, ascites
- Examine for pulmonary HTN – seen with OSA
- Palpable P2, RV heave, elevated JVP, TR
- Examines for gynaecomastia and breast masses in men
- Examines for nipple discharge – if pit. tumor co-secreting prolactin
Abdomen
- Palpate for internal organ enlargement
- Spleen
- Percussion – Castell’s method (percuss lowest intercostal space in anterior axillary line = + if dull on insp), Traube’s space, Nixon method
- Palpation – supine & two handed in RLD position
- Liver – Percuss total liver span (N < 13cm), palpate for hepatomegaly
- Kidneys – bimanual method (balloting)
- Spleen
- Testicular exam for atrophy (seen if associated gonadotropin deficiency or co-secreting pituitary tumor – prolactin & GH)
Lower limbs
- Examine for OA
- Knees – crepitus on passive movement, bony enlargement, varus deformity, pain
- Hip – restriction of internal rotation, abduction & extension, pain
- Examine for proximal myopathy (eg. Quadriceps strength bilaterally)
- Heel pad thickness (measure by radiologic assessment- useful for serial followup)
- Examine for common peroneal nerve entrapment (L4-S1)
- Foot drop (unable to dorsiflex/evert, high steppage gait) and decreased sensation over dorsum of foot & lateral shin. Normal reflexes.
To finish
- Extension of the physical examination
- Glucometer – check BS (associated with DM)
- Urinalysis – for glycosuria
- Recommends colonoscopy – at diagnosis (Endocrine Society, 2014)
- Q 5 years if previous polyp, persistently elevated IGF-1 or positive FHx for colon cancer
- Q 10 years if no polyp and normal IGF-1
- Risk of polyp increased but true risk of ca. is unknown
References: Endocrine Society Acromegaly Guidelines, 2015 • Clinical Examination 6th ed: Talley & O’Connor, 2010

You must be logged in to post a comment.